After Trauma, How Do You Know If It's Acute Stress Disorder, or Something More? A Psychiatrist Explains


After experiencing a major traumatic event — a car accident, a natural disaster, witnessing violence, or learning that someone close to you has been seriously harmed — it's normal to feel shaken. Fear, sleeplessness, a racing heart, or a sense that you're not quite present in your own life: these reactions make sense. Your nervous system is doing exactly what it's designed to do.
But when these responses persist for more than a few days and begin to interfere with how you function, they may point to something more specific: Acute Stress Disorder, or ASD.
This article explains what ASD is, how it's diagnosed, how it differs from PTSD, and what early support can look like.

What Is Acute Stress Disorder (ASD)?
Acute Stress Disorder refers to psychological reactions like anxiety, tension, and fear that people experience in a short time after going through major traumatic events.
These reactions typically last more than three days but no longer than four weeks, essentially an "extended acute stress response".
Common situations triggering acute stress disorder include:
- Personally experiencing disaster events: Such as encountering terrorist attacks or indiscriminate violence, or being in major car accidents, earthquakes, floods, or fires.
- Witnessing firsthand: Seeing others die or suffer serious injury.
- Learning of news: Hearing that someone close experienced a serious accident or traumatic event.
Most people will feel fear, anxiety, or insomnia after experiencing trauma—these are all normal phenomena.
However, if these conditions persist beyond 3 days, with continued intrusive thoughts about the event, anxiety, dissociation, sleep difficulties, or even impact on life or work, seeking professional help and support is recommended.
What Are the Symptoms of Acute Stress Disorder?
Below are common reactions and manifestations when acute stress occurs [1]:
- Trauma re-experiencing: Repeatedly seeing event images, nightmares, or experiencing strong psychological or physiological reactions in related situations. Children may unconsciously reenact event fragments in play.
- Negative mood: Persistent low mood, loss of interest in previously enjoyed things, or inability to feel happiness, sadness, or other emotions.
- Dissociative reactions: Feeling somewhat disconnected from oneself or the outside world, or temporarily unable to recall parts of the event.
- Avoidance tendencies: Deliberately avoiding thoughts, conversations, places, or people and things related to the event.
- Heightened arousal: Difficulty falling or staying asleep; irritability or outbursts of anger; trouble concentrating; being easily startled; a constant sense of being on guard.
Acute Stress Disorder vs. PTSD: What Is the Difference?
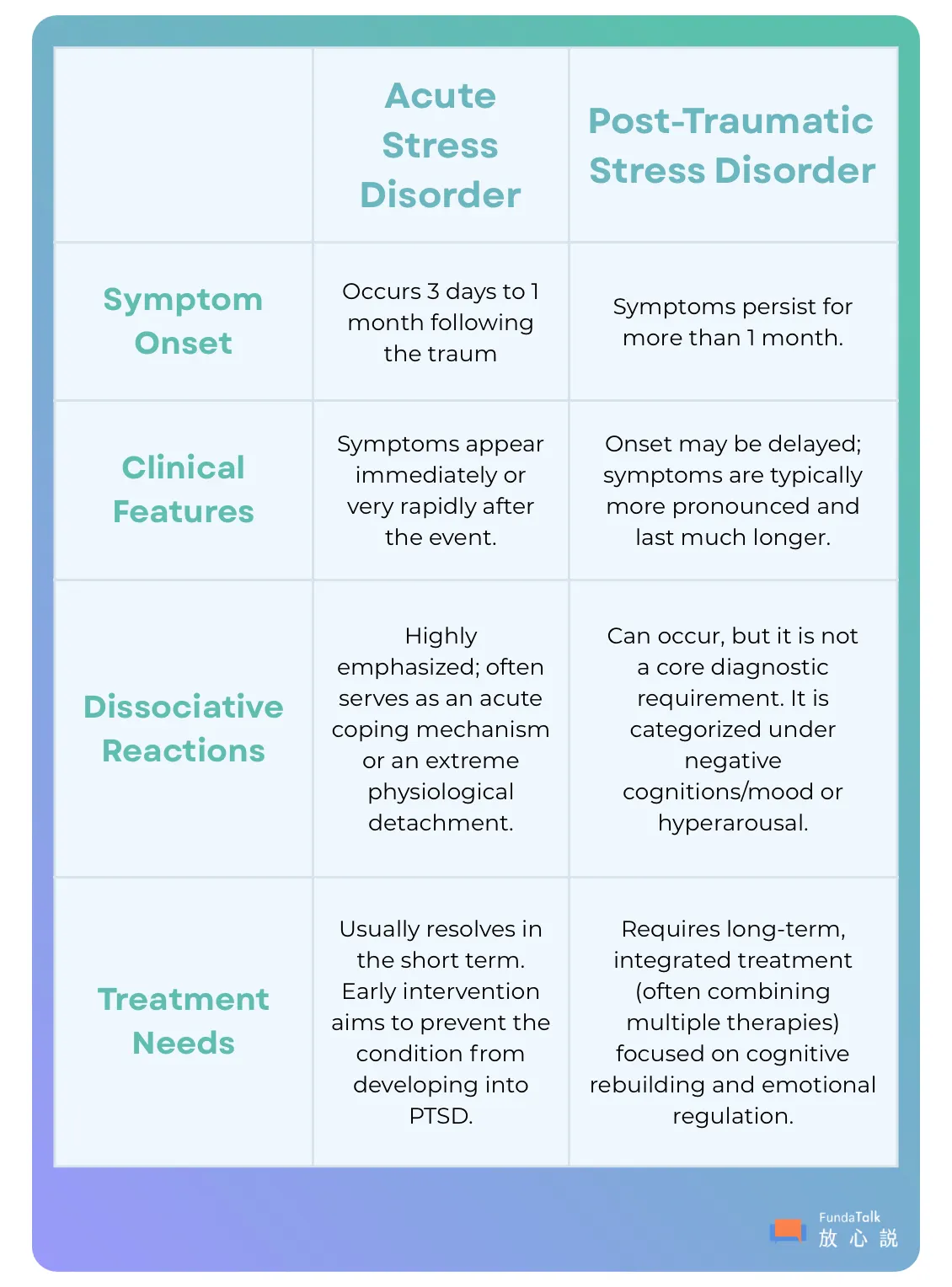
ASD and PTSD share many overlapping symptoms, which is why people often confuse the two. The key differences come down to timing and duration.
ASD is diagnosed when symptoms appear within three days of trauma and resolve within four weeks. PTSD is diagnosed when symptoms persist for more than one month, or when significant impairment continues beyond that window.
In terms of onset, ASD typically develops quickly and acutely. PTSD can have a delayed onset, sometimes emerging months after the event, with symptoms that are often more entrenched and harder to shift.
Dissociation plays a more central diagnostic role in ASD than in PTSD. In ASD, dissociative symptoms are considered a core feature and may reflect the nervous system's acute attempt to cope with overwhelming experience. In PTSD, dissociation can occur but is not a primary diagnostic criterion.
Treatment timelines also differ. ASD often responds well to early, short-term intervention. PTSD typically requires longer-term, more integrated treatment that addresses cognitive patterns and emotional regulation over time.
The relationship between the two conditions matters. If ASD symptoms do not resolve within a month and continue to worsen, that is a sign the condition may be progressing toward PTSD. Early intervention during the ASD window is one of the most effective ways to reduce that risk.
What Increases the Risk of Developing ASD?
Most people recover from trauma without developing ASD, but certain factors can raise the likelihood. These risk factors fall into three timeframes.
1. Before-trauma:
Personal history matters. People who have experienced prior trauma, previously been diagnosed with anxiety or depression, or have fewer social and material resources tend to be at higher risk. Lower educational attainment has also been identified as a contributing factor in research.
2. During the trauma:
Events that involve direct physical threat, violence, or sexual assault tend to produce stronger acute stress responses than other types of trauma.
3. After the trauma:
Recovery conditions shape outcomes. Ongoing anxiety, dissociation, physical symptoms like chest tightness or pain, limited social support, and disrupted living situations all make it harder for the nervous system to return to a regulated state.
How to Support Someone with Acute Stress Disorder (ASD)?
IIf someone you care about is going through this, what you do in the days following trauma can genuinely matter[1].
1. Safety and Basic Needs
The most helpful things you can do are practical and steady. Make sure their immediate needs are covered: housing, food, and daily routines. Help with logistical tasks they may be too overwhelmed to handle, such as filing a police report, contacting an employer, or navigating insurance paperwork. Check in consistently over time, and gently encourage follow-up care if symptoms are not improving.
2. Pay attention to signs of serious distress
Persistent hopelessness, withdrawal, or any indication they may be thinking about harming themselves. If you notice these, do not wait. Encourage them to speak with professional, and offer to help them take that step.
There are also things to avoid, even when your intentions are good.
Do not encourage detailed retelling of the traumatic event within the first 72 hours. Research consistently shows this does not prevent PTSD, and it can reactivate distress during a period when the nervous system most needs stability.
Do not suggest using alcohol, overwork, or avoidance as ways to cope. These approaches may dull discomfort in the short term, but they interfere with the kind of processing that leads to genuine recovery.
Treatment Options for Acute Stress Disorder
Psychotherapy
Cognitive Behavioral Therapy (CBT) is the most evidence-supported treatment for ASD. The focus is not on recounting the event in detail, but on examining how the event has shaped the way a person is thinking about themselves and the world.
After trauma, it is common to fall into thought patterns such as: "This happened because I wasn't careful enough" or "I should have known." CBT helps a person step back from these thoughts, look at whether they reflect reality, and gradually shift toward a more accurate and compassionate understanding of what happened.
For example, a person who keeps thinking "I could have prevented this" might, through therapy, come to recognize: "I was doing my best with what I knew at the time. What happened was not within my control."
Research shows CBT can significantly reduce the frequency of nightmares, intrusive memories, and anxiety, and meaningfully lowers the likelihood of developing PTSD.
Medication
Medication is not the primary treatment for ASD, but it can play a supportive role. When a person is experiencing significant anxiety, sleep disruption, or depressive symptoms during the acute phase, medication may help create enough stability for other recovery processes to take hold. This is always determined on a case-by-case basis in collaboration with a prescribing physician[1].
Conclusion
Acute Stress Disorder is a real and recognized response to overwhelming experience. It is not a sign of fragility, and it does not mean things will not get better. For most people, with time and the right support, they do.
What matters is knowing what to look for, understanding when the response has crossed into territory that warrants professional attention, and not waiting too long to ask for help. Early recognition and timely care are the most reliable ways to protect long-term mental health.
If you'd like to speak with a professional Psychiatrist, you can schedule an online psychiatric consultation here.
Reviewed and Written by Dr. Yun-Chih Chiu, MD

Clinical Specialties
Depression, bipolar disorder, panic disorder, obsessive-compulsive disorder, eating disorders (anorexia and bulimia), psychosomatic conditions, and trauma-related disorders including acute stress disorder and PTSD.
Credentials and Training
Board-Certified Psychiatrist, Taiwan
MD, Taipei Medical University
Senior Resident Physician, Department of General Psychiatry, Taipei City Hospital Songde Branch
Certified Focusing Trainer and Therapist, The Focusing Institute (TIFI)
Member, Taiwan Society of Biofeedback and Neurofeedback
Trained in Mind-Body Axis Awareness Practice
Training in Psychodynamic Psychotherapy
Training in Psychodrama
Further Reading
- About Post-Traumatic Stress Disorder (PTSD): Symptoms, Impact, How PTSD Differs from Depression and Anxiety | Your Brain Remembered "Danger" But Can't Let It Pass
- Rapid Heartbeat, Can't Breathe, Sudden Breathlessness? | Understanding Panic Disorder: Symptoms, Self-Assessment, Effective Relief Techniques
References
- Fanai, M., & Khan, M. A. B. (2023). Acute stress disorder. In StatPearls. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK560815/
- Bryant, R. A., Mastrodomenico, J., Felmingham, K. L., Hopwood, S., Kenny, L., Kandris, E., Cahill, C., & Creamer, M. (2008). Treatment of acute stress disorder: A randomized controlled trial. Archives of General Psychiatry, 65(6), 659–667. https://doi.org/10.1001/archpsyc.65.6.659
More Articles
 )
) )
) )
)